

1/24/2021
There is a non-zero probability that anyone receiving an mRNA-based vaccine against SARS-CoV-2 will experience changes in their DNA in cells “infected” by the encapsulated mRNA. There is also a non-zero probability that people who receive the mRNA vaccine will pass on those changes to some or all of their kids, a genuine concern for some people of faith. Here’s why the non-zero probabilty matters.
We live in a risk-averse world. We want no one to die or get sick “unnecessarily” – i.e., under conditions where the risk of that death or illness could have reasonably been eliminated, or, if not eliminated, at least minimized.
When SARS-CoV-2 entered the human population as a pathogen, most of our species had not seen it. Data from Trevor Bedford dating the age of the SARS-CoV-2 lineage, and my own research points to the fact that non-SARS viruses that were SARS-CoV-2 like may have existed as far back as 2005, or earlier.
If SARS-CoV-2 had entered the species before 2019, it certainly had not gone global – it might have caused a local pocket of pneumonia-related deaths not attributed to anything in particular. In fact, it may have done this many times over the past two or three decades. Because it was deadly, it could not survive long. When the species jump did take hold, sometime in 2019, the virus that made the leap was more transmissible, and perhaps a little less deadly.
The way SARS-CoV-2 creates disease in humans is nefarious. I predicted non-respiratory illness effects in April 2020, when I published my study introducing the concept of pathogenic priming. Sadly, many of the tissue and organ sites other than lung, including parts of our immune system, seem to be impacted by the virus, and our bodies’ immune responses to the virus, likely via the development of autoantibodies to proteins either found in specific organs, or in some cases, ubiquitously found in all cells. Autommunity in so many tissues occur given repeated exposures to the viral proteins in expected given the high level of similarity of the viral proteins to our own proteins – which is why I argued that the parts of the proteins should not be included in any vaccine.
Another question that occured to me in April that I did not have ready answer for the question “What is the probability this virus will cause changes to our DNA?” This question is asked among scientists in the following way: Can we expect that the virus’ RNA genome, or any part of the viral genome, be copied into the human genome as DNA?
Dr. Teresa Deisher is an expert in insertational mutagenesis – the process by which foreign DNAs can enter the nucleus of the cell and become inserted into a person, or animal’s genome. In April, I asked her what the likelihood that the mRNA in an mRNA vaccine, such as Moderna’s vaccine, might by copied into the human genome. Her answer was an educated guess: about the same rate as that of the virus.
Now, many people are asking me the same question. Looking into the availables studies, we find this this study, by Zhang et al., (2020). published by the Whitehead Institute. The study is published on the biorxiv server and as of this writing (1/24/2021) has not been peer reviewed. Nevertheless, the study found that the viral genome can evidently be reverse-translated into DNA, a process that requires a special enzyme called reverse transcriptse. The study suggests that the resulting DNA (complementary to the vira RNA) can be copied in the human genome in two ways: if human cells are infected with HIV virus, the reverse transcriptase enzyme can also act on the SARS-CoV-2 RNA. The SARS-CoV-2 genome was found to be transcribed into some humans cells not infected with a virus providing the reverse transcriptase protein, and the authors of the study speculated that the virus activates a dormant reverse transcriptase enzyme found in our genome in otherwise silenced ancient viruses that long ago called LINES embedded themselves in our ancestors’ genomes.
So the movement of the RNA from the virus to the human genome may be expected to become incorporated in the human genome. What does that mean for the mRNA vaccine, which encodes a stabilized spike protein?
If the Whitehead study results are replicated, then the following must be kept in mind: The SARS-CoV-2 stabilized Spike protein mRNA molecule is an RNA molecule – and as such, it, too could reasonably be expected to picked up by any reverse transcriptase proteins. There are no data ruling out genomic incorporation of the mRNA from mRNA vaccines into the genome of cells in vaccinated people because the issue has not been addressed.
This very question came up during the FDA’s Vaccines and Related Biological Products Advisory Committee meeting considering the Pfizer vaccine (which according to Pfizer contains RNA that encodes (as communicated by Pfizer), a “full mutated spike protein” by two separate attendee (Dr. Moore and Dr. Meissner). Dr. Meissner specifically asked whether fetuses might be at risk of having its DNA changed via reverse transcriptase if the mother-to-be had been vaccinated. Pfizer and other vaccine makers have not directly addressed these questions.
Given the discovery of the Zhang et al. study, which showed it was possible for viral RNAs to modify the human genome, it seems reasonable that is might also occur with mRNA from mRNA vaccines. How frequently this might happen is unknown.
What About the Germline?
To many people, the more imporant question might be whether the vaccine could lead to permanent, heritable changes to the human genome adding new variation that is passed on from generation to generation, i.e., alteration of the germ cells. Germ cells give rise in sperm an egg, and any alteration of cells that give rise to those cells at any stage of development – including, but not especially early fetal development, could lead to the insertion of new DNA into the human genome.
An imporant study that partly addresses the question is the biodistribution study of Bahl et al. (2012), a Moderna study designed to ask the question: where in the body does the encapsulated mRNA from an mRNA vaccine end up? If the tissues where the technology localizes the RNA includes the reproductive organs, it is conceivable that some instances of germline alteration might be possible.
The 2012 Bahl et al. study used mRNAs encoding proteins from influenza viruses, but nevertheless, the principle is demonstrated: the commercial mRNA product was found in the testes.
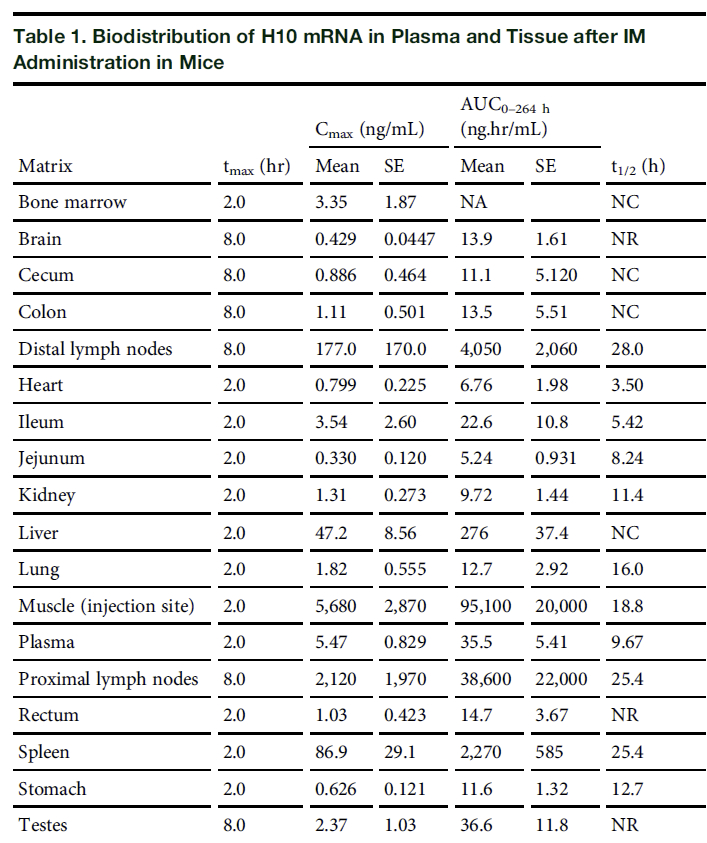
There were no data on the localization of the mRNA to the ovaries, nor to any fetal pups in pregnant mice.
The answer to the question of whether the mRNA vaccines might change the human germ line introducing heritable variation is “likely” – but again, the frequency which which such an event or to whom it might be more likely is unknown.
Neuroscientist Chris Shaw recently discussed this study with Del Bigtree on The Highwire, focusing primarily on the issue that the viral protein was found in the brain, and can be expected to induce the innate immune response in the brain, potentially contributed to microglial activation, immune cells in the brain that are stimulated to respond to viral infections or other foreign substances.
The question of whether you should be concerned or not is a personal one: if your creed, or religion, or personal desire to not have your own genetic lineage forever altered, you might favor approaches to addressing COVID19 infection that keeps viremia to a minimum, such as treatments.
However, if you believe that evolution makes sense of variation wherever its source, and are comfortable with the idea that your descendents might express COVID19 spike proteins, then either the infection or the injection might be your favored route.
However, we have learned from Dr. Anthony Fauci that the mRNA vaccines might not actually confer immunity to SARS-CoV-2 in a way that prevents transmission – and now also from Dr. Fauci that current vaccines might not prove effective against new variants.
In times like this, people must search deeply in their own constitutions and moral compass and determine for themselves which of two or more unwelcome paths they might prefer.
Thankfully, however, we now know that COVID19 viral infection likely confers immunity at least as long as the vaccine – meaning a willful injection with vaccine following prior COVID19 diagnosis might only serve to double the risk of genome and germline alteration. Similarly, initial exposure to a vaccine might cause vaccine induced enhanced viral infection, as described by this paper in the journal Vaccines from 2009.
As an evolutionary biologist, I am not a fatalist. For me, the future brings changes based on the conditions in which we find ourselves, and our decisions given what we know about those conditions. In discussions with people who hold sincere religious beliefs, it seems that for some people who intend to reproduce, a natural course leaving outcomes to fate can be maintained only by eschewing the vaccine, preventing double jeopardy of genomic alterations. For others, faith in the necessary outcomes will help them avert their fears, placing their destiny in the hands of God.

It is a reality that those who have designed these vaccines have created a tortuous set of conditions by the very nature of the vaccine design. Perhaps the best path forward is to provide feedback on their commercial product and provide feedback on treatment options such as Ivermectin, which the NIH has now updated to leave as a choice between a physician and their patient (See FLCCC.net). Ivermectin will never cause changes to our genome or germline.
James Lyons-Weiler is the CEO/Director of The Institute for Pure and Applied Knowledge.
https://phys.org/news/2020-01-rna-effect-dna.html
Thank you, Dona, interesting. Epitranscriptomics!
Thank you for — as usual — an honest, balanced presentation of the facts that allows people to make their own decisions based on their own worldviews.
You’re welcome, Rachel. So much at stake for so many – it’s important for frank consideration free from ambition.
This is terrifying. We are literally being forced into becoming GMOs.
Thanks, excellent.
FWIW, there is concern that vaccinating shortly after recovery from COVID can cause more serious reactions:
“Florian, we are seeing people who were PCR positive more than 90 days ago badly responding to first dose of Pfizer vaccine (severe side effects last for weeks).
I started to recommend Abs test before taking the shot.
Any standard guidance may I double check for such cases? Thanks”
https://twitter.com/DrSusanNasif/status/1350445813579853825?fbclid=IwAR0EDlci3aGjTsCjbs3hfVh_5ryedQFjMClCkMJ6Luxe7cw-50eOR67cz0A
“When the species jump did take hold,sometime in 2019….”
Are you implying Sars-Cov-2 is zoonotic in origin and not bioengineered?
I’m saying that I found a SARS-CoV-2 like spike protein in a sequence published in 2005 (HKU-3-3).
That does not mean it’s the same lineage that SARS-CoV-2 that made the leap into humans and is causing
COVID19. There is insufficient evidence in my view for laboratory modification. Most likely
scenario is lab escape, as the many times SARS escaped. See the articles on the origins of the
virus in this blog including https://jameslyonsweiler.com/2020/02/15/coronavirus-origins-anatomy-of-a-scientific-inference/.
Good article here:
https://cienciaysaludnatural.com/estudio/why-covid-19-vaccines-might-affect-fertility/
Author: Roxana Bruno, Biochemistry PhD in Immunology.
[Long and detailed but highly readable.]
… This modified RNA therapy platform is totally new, it is an experimental form of inoculation of foreign genes into the human body that cannot be called “vaccination” since it does not involve administering attenuated or inactivated pathogens as simple antigens that stimulate immunity. It is the inoculation into the human body of injectable synthetic gene variants, so that they can penetrate into human cells and make them produce the spike (S) protein of the virus. This represents a true transgenesis experiment, never before performed in the history of mankind in order to confer immunity against human-transmitted infectious-contagious diseases. …
Thanks, they are trying to wipe out the human race
JB, thank you for adding this clarification. The FDA did not approve “it” as a vaccine. It’s not a vaccine, but an experimental gene therapy.
The unsuspecting (dare I say, ignorant) masses think it’s a vaccine.
I appreciate James Lyons-Weiler’s work. I have been following it for a while. Nonetheless, I do not think it is asking too much to ask him to share with us why he–an expert on these matters–is incorrectly referring to BNT-162bt–as a “vaccine.”
At least he mentions Ivermectin at the very bottom of the article. Isn’t it generous that the NIH is “allowing” the use of Ivermectin as a choice left up to the physician and patient? Of course, it’s a little late for the people to find out that all they have to do to treat covid is pop a couple of Ivermectin–a completely harmless, common drug. It will take untold numbers of deaths and injuries for them to figure out that they don’t need to subject themselves to the dreadful BNT-162bt.
It is only out of fear, and because they believe what their TVs say, that people are allowing themselves to be injected with an experimental gene therapy whose long-term effects are completely unknown. We can already see that the short-term effects are extremely negative. https://prezi.com/i/byzl22mqwfaa/experiences-following-cvv/
This is a sad world we live in.
Joe,
Here’s more info on Ivermectin (you likely have seen it).
Regarding what to call it, I get that point, if it’s a gene therapy it should be regulated as such.
Unfortunately, I am not (yet) endowed with the power to unilaterally reclassify these products.
Dr. Lyons-Weiler I am impressed by your careful work. May I post the 8 hour webinar on my brighteon site. I screen captured it and would like it to be widely seen. I will include references to your site and where you can be supported. I make no money off reposting them. Also, as an evolutionary biologist, I think you will find this conversation very interesting. It seems the math bears out his claims. Also on this post is a link to a talk given to a group at the NIH on a similar topic which appears very solid to me. Best regards. https://kgov.com/christopher-rupe
Rob, Thank you!
Each part of the 8-hour webinar will be made available for general download and distribution, yes.
Working on that, watch this blog for news on how to access.
Dr. J
Regarding the 94.5% effectiveness, Del Bigtree posted this report estimating it at 19-29%. Discrepancies and wildly vague information from health departments and the drug makers themselves about new #Covid19 vaccines continue to run rampant. From mixing and matching different shots to delaying the second dose, some mainstream medical journalists are demanding to see the raw data. Effectiveness could actually range from 19-29% — far below 50%. Will the pharmaceutical companies release the raw data?
Video Source: https://thehighwire.com/videos/science-junked-as-covid-vaccine-rollout-falters/
Watch full episodes or support The Highwire here: https://thehighwire.com
Thank you for this insightful article, James. Your work is much appreciated!
Adding to the long list of risks and unknowns that you’ve already stated, I wonder if you are aware of the issue of “RNA integrity”? Specifically, documentation submitted by Pfizer to various regulatory agencies indicates that the mRNA in their vaccine is only ~50-80% intact and accurate for coding for the spike protein in the current SARS virus. So it seems logical to assume that as much as 50% of the time, proteins other than the desired one are being produced in a vaccinated individual. If this is true, what implications might that have?
A second concern with these vaccines is the persistence and/or proliferation of extracellular RNA. Extracellular RNA is a known promotor of inflammation, coagulation, and neurological pathologies. The fact that the mRNA in these vaccines has been modified to resist degradation through normal enzymatic processes may explain some of the adverse events that are being reported.
Would be awesome to have diagrams or a simple video summarising the possible interaction of mRNA from a vaccine interacting with DNA. Most laypeople like myself are simply assured by physicians that since the DNA resides in the nucleus, it cannot be touched at all by the synthetic RNA, which will remain in the cytoplasm.
The layperson has no comeback to this, even just to say “we don’t know”, because it is presented as a fact as concrete as the earth is round.
An example from HIV –
Hope it helps!
If mRNA could be integrated in our genomes, considering that our cells contain millions or even billions of mRNA at all time in our ~80 years of existence, our genomes would be filled with pseudogenes caused by this integration.
But they don’t. Because retro-transcriptases (RT) only integrate specific sequences (i.e. HIV RT are specific for HIV integration). Using artificial models of tremendously over-expressed RT like is used in the paper by Zhang et al. does not represent an adequate model to study in-vivo phenomenon.
There is no question that mRNA can be integrated into our genomes. HIV and all retroviruses demonstrate that.
Regarding your point about millions of years, check out the role of viral incorporation during mammalian evolution,
e.g.,
https://onlinelibrary.wiley.com/doi/epdf/10.1111/gtc.12278
https://www.sciencedaily.com/releases/2016/07/160713100911.htm
https://www.pnas.org/content/117/1/610
https://www.sciencefocus.com/the-human-body/virus-human-evolution/
The Zhang shows a proof of principle.
Absolutely not. We are not talking about HIV integrating HIV or LINE who integrate LINE. We are talking about retroviruses who would suddenly go out of their way to integrate a random mRNA that is not its target.
If that was the case, we would see pseudogenes across the our entire genomes, which would be really easy to identify thanks to their poly-A signature.
Zhang and al. study is no where near a proof of principle, since they are using are completely artificial model that has the active retro-transcriptase expression in one cell equivalent to the amount found normally in an entire person.
In addition, finding reads flagged as “chimeric” using RNA-seq yield high levels of false positive, and not a single one of these reads were validated using an alternative sequencing method, which any serious study would do.
To note, no “chimeric” sequence were actually found in patient samples, only artificial cellular models.
Extrapolating perfect condition in vitro experiments to human phenomenon is dangerous and dishonest.
So is extrapolating perfect theoreticals and assuming that genetic material will necessarily always behave exactly the way we want it to.
The difference is, you seem to be suggesting that we should act based on the unproven assumptions, as opposed to acknowledging the unknowns and practicing the precautionary principle.
That is not correct. You’re confusing “could be” or “can be” with “definitely are, in every instance.”
We know, for instance, that some vaccines can induce autoimmunity. They don’t always. But they can. And therefore, autoimmunity is a risk — and one we can’t adequately mitigate without understanding WHY they induce autoimmunity when they do and don’t when they don’t.
Likewise, mRNA from the vaccines could possibly be reverse-transcribed into the cells. Does it usually? Not likely. But that doesn’t change the fact that it COULD or CAN — and we don’t know what circumstances might make that happen.
Rachel, agreed. That said, “non-zero probability” (on my part) is not a very precise estimate, but that’s due to a lack of studies conducted to provide more precise arguments by those bringing these vaccines to the public!
Since it has never been observed, suggesting such extravagant mechanism is irresponsible. Demanding that one proves the non-existence of something is logically fallacious.
You are more likely to win the lottery while being in a plane crash while being struck by lightning than having the mRNA reverse-transcribed.
This isn’t science, it is fan fiction.
Last I checked, absence of evidence still wasn’t evidence of absence.
It’s easy to “not observe” things you’re not looking for, whether or not they’re there to be seen.
It is easy to invent mechanisms when you absolutely don’t have the intention to look for it.
The burden of proof lies with the person making the claim.
It would impoverish science massively if the only person who tested an hypothesis was the person who generated it.
So you are aware that you are wildly extrapolating and distorting the research results you are presenting as “scientific evidence” to support your pseudoscience but you don’t care because it generates clicks.
Great. Keep generating unnecessary fear for a technology that is clearly much safer than the disease it protects you from.
The distortions are not mine.
Hmmm…”a technology that is clearly much safer than the disease…” Really? Tell that to the widow of the doctor in Florida whose platelet count dropped to zero just 3 days after getting the vaccine and died 2 weeks later from a hemorrhagic stroke. His doctors were never able to get his platelet count up. Or the x-ray tech in California who ended up intubated several hours after vaccination this past week and died 4 days later in renal failure? Talk about “wildly extrapolating and distorting the research.” Pot, meet kettle. We will not know for months, if not years, whether or not this approach was worth the cost or safer than early outpatient therapy. And if the NIH, FDA and the CDC had not hampered physicians in treating their patient’s with early outpatient therapy, this disease would not have been as deadly to so many people. But then again, if there had been a treatment available for Covid-19, the emergency use authorization for the vaccine would have been terminated. Gee, we can’t have that!
James,
Just doing a cursory search on Microglia & mRNA turned up the below study on Cell Reports
_____
CERVO Brain Research Centre and Department of Psychiatry and Neuroscience, Faculty of Medicine, Laval University, Que ́bec, QC
TITLE
“Diverging mRNA and Protein Networks in Activated Microglia Reveal SRSF3 Suppresses Translation of Highly Upregulated Innate Immune Transcripts”
https://www.cell.com/cell-reports/pdf/S2211-1247(17)31710-2.pdf
_______
It seems to mirror what the Geert Vanden Bossch had presented as his appeal to cease the mass vaccination campaigns.
I do not understand the study but those with integrity whom do… seem like they should be talking about it’s contents, especially given the presence of the mRNA in the brains in the above Moderna 2012 study.
Thoughts?
PDB – I don’t see the connection between the CERVO study you posted and the concern over mass vaccination against SARS-CoV-2?